Instead of maintaining high-intensity statin to prevent secondary complications in atherosclerotic cardiovascular diseases, controlling statin intensity according to LDL-cholesterol treatment targets can produce similar treatment effects, Korean researchers said.

A research team led by three Severance Hospital cardiologists -- Professors Hong Myeong-ki, Hong Sung-jin, and Lee Yong-joon – said Friday that a treatment that controls statin intensity to suit low-density lipoprotein cholesterol (LDL-C) treatment targets in atherosclerotic cardiovascular diseases is equally effective to high-intensity maintenance therapy while lowering statin-related side effects.
Cardiologists usually use two strategies in administering statin to prevent secondary complications and lower LDL cholesterol in patients with atherosclerotic cardiovascular disease. One is the “treat-to-target” strategy, which sets LDL-C treatment targets and controls statin intensity according to them. The other is to use high-intensity statin regardless of LDL-C levels,
The high-intensity statin strategy is convenient as it does not need to control statin intensity. However, individual response to statin can vary, and the long-term use of high-intensity statin can result in side effects, including muscle pain, liver damage, and diabetes.
On the other hand, the treat-to-target strategy makes customized treatment possible and reduces the side effects of the high statin-intensity strategy. However, no studies have compared the two statin treatment strategies.
The research team conducted the LODESTAR study, in which they randomly assigned 4,400 cardiovascular patients treated for myocardial infarction, stroke, or coronary revascularization at Korean hospitals from September 2016 to November 2019 into two groups at a rate of 1 to 1 – the treat-to-target group administered with a controlled statin to suit the LDL-C target of 50-70g/dL, and the high-intensity statin group, and followed them for three years.
As a result, the treat-to-target showed an LDL-C level of 69.1mg/dL, little different from the high-intensity statin group’s 68.4mg/dL.
On the other hand, in the statin intensity-controlled group, they used 54 percent of high-intensity statin and 43 percent of medium-intensity statin, reducing the use of high-intensity statin to lower LDL-C levels in about half of the patients.
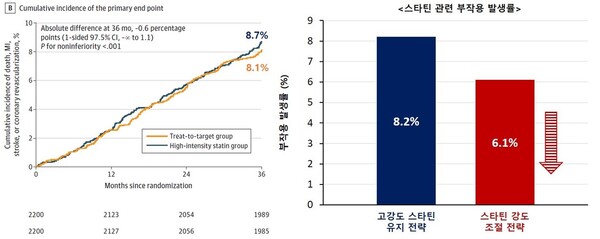
During the three-year follow-up period, in comparing clinical outcomes, such as death, myocardial infarction, stroke, and coronary revascularization, there were not many differences between the controlled group’s 8.1 percent and the high-intensity group’s 8.7 percent.
In contrast, in statin-related side effect occurrence, such as new diabetes, liver, rises in liver and muscle enzyme levels, and end-stage renal failure, the controlled group showed 6.1 percent, far lower than the high-intensity statin group’s 8.2 percent.
The research team explained the LODESTAR study had shown that the treat-to-target strategy produced similar treatment effects to the high-intensity maintenance strategy while lowering side effects, expecting the former to emerge as a new alternative treatment strategy.
“We confirmed that in treating cholesterol in atherosclerotic cardiovascular diseases, statin intensity-controlled strategy does not pull down efficacy while lowering side effects,” Professor Hong Myeong-ki said. “The study is significant by confirming the clinical usefulness and stability of the statin control strategy.”
The study was published in the latest issue of the Journal of the American Medical Association (JAMA).