Song Kyo-young, Professor of the Department of Gastroenterology at the Catholic University of Korea Seoul St. Mary's Hospital
Surgery for stomach cancer involves three main techniques. The first is to remove enough of the stomach to contain the cancer; the second is to extensively remove the lymph nodes surrounding the stomach for possible metastasis; and the third is to safely attach the small intestine to the remaining stomach or esophagus.
During this process, lymph node dissection is a critical skill that can significantly impact the outcome of the surgery. If insufficient lymph nodes are removed, metastatic lymph nodes may remain, allowing the disease to recur. On the other hand, if it is done excessively or carelessly, it can lead to surgical complications, including damage to major blood vessels.

Lymph nodes (also known as lymph glands) are small nodules that play a crucial role in the immune system, which defends the body by eliminating foreign substances, including bacteria that have invaded the body. In cancer patients, lymph nodes fight against foreign cancer cells. However, when they become occupied by cancer cells, they lose their function and become a route for the cancer cells to spread.
Lymph nodes are found throughout the body, including the stomach, which usually has a large number of complex lymph nodes. In patients with stomach cancer, cancer cells originate in the stomach. Still, over time, they migrate to the lymph nodes around the stomach, and lymph node metastasis begins in early-stage stomach cancer as well as in more advanced stomach cancer, such as Stage 2 or 3.
As the disease progresses, cancer cells that have metastasized to the perigastric lymph nodes travel to lymph nodes further away from the stomach, including the para-aortic lymph nodes, axillary lymph nodes, inguinal lymph nodes, and cervical (neck) lymph nodes.
The lymph nodes located near the stomach are referred to as regional lymph nodes, while those farther away are classified as distal lymph nodes. While regional lymph nodes can be expected to improve survival when resected, distal lymph nodes do not have the same effect on survival when resected. They are treated as distant metastases, such as liver metastases, lung metastases, and metastases to other organs.
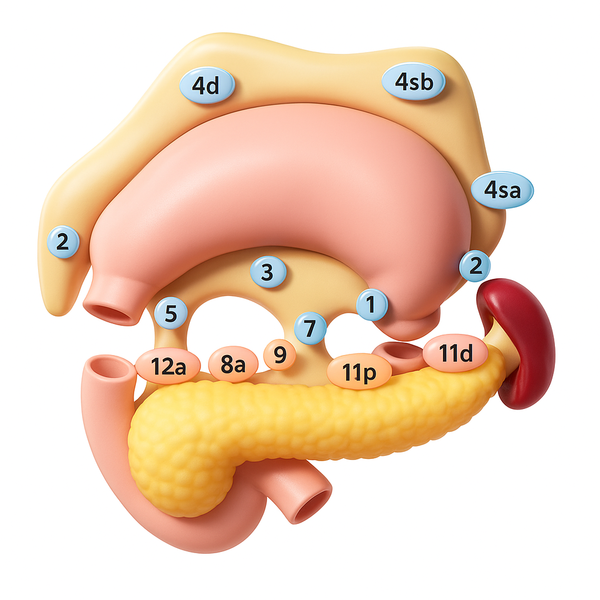
Regional lymph nodes are divided into primary lymph nodes, located near the stomach, and secondary lymph nodes, which are positioned slightly farther away. They are uniquely numbered from 1 to 12 according to the anatomy of the stomach. For example, the greater curvature area of the stomach is number 4, the lesser curvature is number 3, and the area close to the duodenum is number 5 or 6. Generally, it is standard to remove a sufficient number of lymph nodes from both the first and second lymph node groups during surgery, a procedure known as D2 lymph node dissection, which is considered standard surgery.
Despite extensive lymph node dissection, there is no need to worry about immune system problems. However, the larger the scope of the surgery, the higher the risk of postoperative complications or sequelae. Surgical site adhesions, bleeding, and postoperative pain can be problems.
Therefore, to minimize these problems, it has become necessary to vary the extent of lymph node dissection depending on the stage of the gastric cancer patient. This is based on the experience that the lower the stage, the lower the frequency of lymph node metastasis, and conversely, the more advanced the disease, the higher the frequency of lymph node metastasis and the broader the scope of metastasis.
Recent surgical trends follow the concept of so-called tailored treatment, with aggressive and extensive lymph node dissection in advanced gastric cancer and selective lymph node dissection in early gastric cancer.
It means that for early-stage stomach cancer, a reduced surgery is performed to remove mainly the primary lymph nodes while leaving most of the secondary lymph nodes, which are less likely to metastasize. The aim is to reduce the risk of complications or sequelae from extensive lymph node dissection.
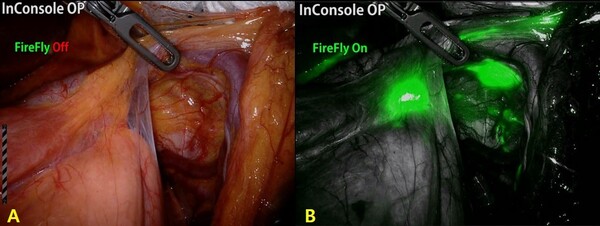
Of course, it is essential to spare the lymph nodes that don't need to be removed, but it is even more important to do a thorough job of removing the lymph nodes that do. To perform these lymph node dissections effectively, newer techniques have been developed that provide a clearer view of the lymph node's path of travel.
After the patient is put under general anesthesia, an endoscope is used to inject a fluorescent substance into the cancerous tissue. This substance travels along the lymphatic vessels to the lymph nodes surrounding the stomach. A special camera is then used to detect the fluorescent substance and locate the lymph nodes that are likely to metastasize.
Stomach cancer surgery is an area of continuous technological advancement.
From open to laparoscopic and robotic surgery, the evolution is still underway to personalize treatment using various technologies that help make surgery more efficient and safe, while minimizing side effects and improving survival rates.
Related articles
- [Contribution] ‘Anemia’ is the most common change after stomach cancer surgery
- [Contribution] Immunizations for gastric cancer patients
- [Column] Why are post-operative anticancer chemotherapies different in stages 2 and 3?
- [Contribution] What’s the appropriate time between diagnosis and surgery of stomach cancer?
- Stomach cancer survival highest with chemo within 6 weeks of surgery