Research findings suggest that ginkgo biloba extract inhibits the aggregation of beta-amyloid, a protein associated with the development of Alzheimer's disease, not dementia. This study is notable as it is the first to demonstrate the oligomerization-inhibiting effect of ginkgo biloba extract when administered alone.
Professor Yang Young-soon of the Department of Neurology at Soon Chun Hyang University Hospital, who is also the insurance director of the Korean Dementia Association, recently published the clinical results of the study, titled “Efficacy of Ginkgo biloba extract in amyloid PET-positive patients with mild cognitive impairment,” in the international neurology journal, “Frontiers in Neurology.”

Professor Yang's team selected 64 MCI (mild cognitive impairment) patients who tested positive on amyloid PET scans. They administered 240mg of ginkgo biloba extract daily to 42 patients and existing cognitive enhancers (including omega-3 and choline precursors) to 22 patients for 12 months, comparing their progress. The ginkgo biloba extract used was Ginexin from SK chemicals.
The researchers comprehensively observed changes before and after treatment across multiple indicators: the blood-based biomarker MDS-Oaβ (Multimer Detection System–Oligomeric Amyloid β); the standardized cognitive assessment tool K-MMSE-2 (Korean version of the Mini-Mental State Examination); the CDR-SB (Clinical Dementia Rating – Sum of Boxes), indicating the clinical severity of dementia; and K-IADL (Korean version of the Instrumental Activities of Daily Living scale), and NPI (Neuropsychiatric Inventory) to comprehensively observe changes before and after administration.
The study results confirmed an effect in lowering MDS-Oaβ levels, which indicate the degree of beta-amyloid aggregation.
The MDS-Oaβ level in the group administered ginkgo biloba extract decreased by 0.08 ng/mL, from 0.88 ng/mL to 0.80 ng/mL. In contrast, the control group showed an increase of approximately 0.02 ng/mL, rising from 0.89 ng/mL to 0.91 ng/mL.
MDS-Oaβ is a biomarker quantifying the tendency toward “oligomerization,” the earliest pathological stage of Alzheimer's disease. Lower levels are considered more likely to inhibit disease progression.
Beta-amyloid, when undegraded, becomes increasingly toxic over time as its structure changes upon aggregation. Initially existing as small fragments (monomers), it gradually forms small, sticky clusters called oligomers. Subsequently, it progresses through a fibrous form (protofibrils) and eventually deposits in the brain as large masses, known as beta-amyloid plaques. These plaques are known to cause brain cell damage and symptoms of dementia.
Oligomerization is the first step leading directly to beta-amyloid plaques, which are directly linked to dementia. Drugs that slow the tendency to form oligomers are therefore considered a crucial therapeutic option for inhibiting dementia progression.
“Beta-amyloid exhibits the greatest toxicity to brain cells during the oligomer stage, and once aggregation begins, the disease tends to progress rapidly,” Professor Yang explained. “The reduction in MDS-Oaβ levels demonstrates that drug therapy can manage dementia progression. This holds significant promise not only for treating subjective cognitive impairment or early mild cognitive impairment but also for preventive dementia management.”
Ginkgo biloba extract enables patients to maintain cognitive function and daily living
The research team analyzed the K-MMSE, CDR-SB, and K-IADL indicators together to comprehensively evaluate cognitive function and daily living capabilities.
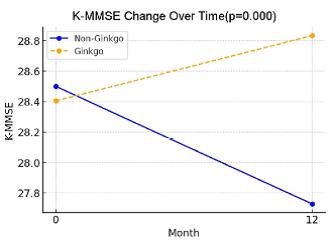
The K-MMSE is a widely used screening tool for dementia that quantifies cognitive functions, such as memory, orientation (the ability to recognize time, place, and people), and attention.
In the study, the ginkgo biloba extract group showed a 0.4-point increase from 28.4 to 28.8 points, whereas the comparison group exhibited a statistically significant decline in cognitive performance from 28.5 to 27.7 points.
On the CDR-SB (Clinical Dementia Rating – Sum of Boxes), a scale comprehensively evaluating independence in daily activities, such as meals, hobbies, and communication, alongside cognitive decline levels, the ginkgo biloba extract group showed a slight decrease in score (0.845 → 0.835) and a stable course. In contrast, the comparison group showed no significant change and remained stagnant.
In the K-IADL (Korean Instrumental Activities of Daily Living) index, which measures functional independence in real-life settings, the ginkgo biloba extract group showed a 0.8-point improvement from 3.4 to 2.5 points. Conversely, the comparison group increased from 3.0 to 3.5 points, a rise of 0.6 points. Lower scores on the CDR-SB and K-IADL indicate better functional status.
A clear difference was also observed in the conversion rate to Alzheimer's disease among treated patients. In the comprehensive clinical assessment, no cases converted from mild cognitive impairment to Alzheimer's disease over 12 months in the ginkgo biloba extract group, whereas three out of 22 patients (13.6 percent) in the comparison group were diagnosed with Alzheimer's disease.
Regarding adverse reactions, no serious adverse events were reported in either the ginkgo biloba extract monotherapy group or the comparison group. Mild adverse reactions such as diarrhea, headache, nausea, and dizziness were observed in some cases, but none required discontinuation of treatment.
Possibility of intervention at mild cognitive impairment stage, drawing attention as realistic early treatment alternative
This study is highly significant not only for confirming indicators that ginkgo biloba extract can slow the progression of oligomers—the early stage of beta-amyloid aggregation known to cause dementia—but also for demonstrating that this leads to a reduction in the actual Alzheimer's conversion rate.
“Typically, 10-20 percent of amyloid PET-positive MCI patients progress to dementia within a year. However, no cases of progression to Alzheimer's disease were observed in the group where beta-amyloid aggregation was inhibited,” Yang explained. “This study confirms the link between ginkgo biloba extract's beta-amyloid aggregation inhibition effect and the onset of Alzheimer's disease.”
Ginkgo biloba extract is the only compound among drugs used for early treatment, such as mild cognitive impairment, whose efficacy has been confirmed at the beta-amyloid oligomer stage. Choline-based drugs, which work by inhibiting the breakdown of the neurotransmitter acetylcholine, do not directly affect beta-amyloid. In this study, the comparison group also showed increased levels of MDS-Oaβ, indicating a tendency toward oligomerization.
“Acetylcholine-acting agents used to treat mild cognitive impairment are medications that improve memory and attention, which decline with reduced brain function. They suppress symptoms and assist with daily functioning,” Yang said. “Therapeutics targeting beta-amyloid oligomerization, known to cause dementia, could serve as a catalyst to shift the treatment paradigm for mild cognitive impairment from ‘symptom improvement’ to ‘progression inhibition.’”